
Child Protection in the Age of COVID-19: What is the Data Telling Us?
As an ever-increasing number of industrial and developing countries fight to slow the spread of the coronavirus pandemic (COVID-19) by putting their economies into a coma/hibernation and by locking down their citizens to reduce social contact, what does this mean from a child protection perspective? Specifically, how is all this impacting, or will impact, on the protection of children in developing countries? I set out to write a blog on child protection more broadly and how the global child protection response, now and with an eye to 2030 and the Sustainable Development Goals (SDGs), may be impacted. However, the data that could give us a complete picture is just not available. This blog is an attempt to estimate the potential size of the problem using as an indicator the number of children who may be orphaned (losing one or both parents) to the pandemic or who may need some form of psychosocial intervention. At the end of the blog is a round-up of news and updates from some of the key international child protection organisations and networks.
While the psychosocial, political and economic damage of the pandemic is being felt in almost all nations, it is at the household level that it is, or will, be most acute. For many children in developing countries (as well as children in socially isolated and economically poor families in middle and upper-income countries), their world is literally collapsing in around them. The pandemic will usher in a tsunami of misery in a variety of ways.
Children in developing countries will be hardest hit for obvious reasons, such as heightened poverty and the poor or fragile state of their health systems. A particular burden for children living in overcrowded households and communities is that they, along with their parents, will struggle to practice social distancing, one of the major tools used in industrial counties to hold back the virus. Also, the absence of clean water and sanitation means that the core message of ‘wash your hands’ will also be incredibly challenging to apply practically.
But a major driver of the pandemic in developing countries will be the simple fact that there are more children growing up in these countries and more households with both children and older people living together. For example, 80 per cent of countries in Africa and Asia include at least one child under 15 years of age whereas it is less than 30 per cent of countries in Europe. Compounding this situation, in Africa and Asia more households include both a child under 15 years of age and an older person aged 60 years of age or over. A stark example of this is in Senegal, where 37 per cent of households have a child under the age of 15 and an older people over the age of 60. In the Netherlands, in contrast, it is only 0.2 per cent.
However, given the limitations of the data available at this point in the epidemic, particularly mortality rates for specific age groups, such as those in the parenting age bracket, and given that the global burden of the virus is still primarily in industrial countries, we have little knowledge about the impact of the pandemic in developing countries. There is simply not enough qualitative or quantitative data to generate concrete estimations.
But we know that adults of parenting age are dying. We know that these deaths create orphans. We know that children who become orphaned are at heightened risk of a range of protection violations. This is one of the many lessons we continue to learn, from the AIDS crisis which, as of 2018, had created just under 15 million orphans.
We also know that children who live in households where a sibling, parent or relative has died are a high priority for psychosocial interventions. Well designed, targeted, age and gender responsive psychosocial programmes are a proven and effective tool for reducing the psychosocial trauma children often face in response to such a loss.
Counting the mortality rates of adults and children, particularly in resource poor countries where child protection services are limited or non-existent, provides a useful indicator for estimating the number of children requiring psychosocial support as part of the broader humanitarian response to the pandemic.
Because we know this, the number of children who may be orphaned (losing one or both parents) to the pandemic or who may need some form of psychosocial intervention can be an indicator of the impact, albeit a crude one.
Before looking at what the COVID-19 data may be telling us about this pandemic and child protection, let’s take a brief look at the data on orphans globally. According to UNICEF there are around 140 million orphans, defined as children under the age of 18 who have lost one or both parents. This includes 15.1 million children who have lost both parents. Most orphans are living with a surviving parent or grandparent, or other family member. The Better Care Network estimates there are 8 million children in residential institutions, but 80 per cent of these children have a living parent, the majority of which could be reunited with their families given the right support. As of 2018, it is estimated that approximately 14.9 million children under the age of 18 have lost one or both parents to AIDS.
At the time of writing this blog John Hopkins University was documenting around 1 million cases of COVID-19 in 180 countries, of which approximately 50,000 people had died and 200,000 people had recovered. The overall mortality rate was just over 5 per cent. Infection and mortality rates by age group were not included in this data. This is part of the reason why precise estimates of the case fatality rates are impossible at present.
Further, as noted by the Brookings Institution in a recent article, the final shape of the pandemic is unclear. It could end up being large or small depending on the time frame, the geographic scale, and the demographic composition of the population affected. For a concise overview of why predicting mortality of this pandemic is near on impossible, see a recent article by the Lancet. That doesn’t mean that the exercise of trying to estimate the number of children who may be orphaned shouldn’t be undertaken.
For the purpose of the exercise I have used three data sets. The first is the population size of adults aged 20-49 in three world regions: Least Developing Countries (LDC); Sub-Saharan Africa; and developing countries, excluding China, in East Asia and the Pacific. UNICEF’s 2019 State of the World Children’s Report, records the total population for these three regions. The assumption is that this age group is most likely to be of parenting age and be the major caregivers of children under the age of 18.
Of course, with child marriage still prevalent in many countries, with 12 per cent of girls marrying by the age of 15 and 39 per cent marrying by the age of 18 in least developed countries, there are parents less than 20 years of age. Conversely, with intergenerational marriage still a common practice in some countries, there are children under the age of 18 growing up in families where one parent is over 50 years of age (almost always the father). However, for simplicity’s sake, I have not included these age groups in this exercise.
I calculated the number of adults in this age group for the three regions by using a great tool provided by the UN Department of Economic and Social Affairs.
The second set of data is the possible number of deaths in this age group. For this I have used as a guide the data from Worldometers available at 29 February 2020. Table 1 shows the global mortality rate for COVID- 19 infections based on nine age groups. More recent data on mortality rates per age group is not available.
Table 1:
Age Mortality rate
0+ years old 14.8%
70-79 years old 8.0%
60-69 years old 3.6%
50-59 years old 1.3%
40-49 years old 0.4%
30-39 years old 0.2%
20-29 years old 0.2%
10-19 years old 0.2%
0-9 years old no fatal
Collapsing the three age groups of 20-29, 30-39, and 40-49 reveals a small mortality rate in the age group 20-49. For this exercise I am using two mortality rates for this age group: 0.5 per cent and 1 per cent to show that even a small mortality rate in the parenting age bracket could have severe consequences for children.
The third set of data is the fertility rate (live births per women) in the three regions, as per the UNICEF report noted above. The data for the East Asia and the Pacific was difficult to tabulate. However, the discrepancies in total population and age groups are minor. Table 2 shows this data.
Table 2:

The formula for arriving at the number of potential orphans and / or children requiring some form of psychosocial support is calculated by multiplying the mortality rate of adults by the fertility rate for the region and grouping. The overriding assumption is that one death in the parenting age bracket will result in x number children being orphaned. For example, the death of one adult of parenting age in Sub-Saharan Africa, which has a fertility rate of 4.7, will result in 4.7 orphans.
This is a crude calculation but is readily available and requires close monitoring by the child protection sector, particularly in terms of planning the child protection dimensions of the humanitarian response to the pandemic.
I made a few further assumptions: First, infections rates across the three regions will be uniform. Second, the mortality rate for adults in the parenting age bracket will be one per cent or less. The exercise does not factor in a higher mortality rate, which is highly plausible given the higher levels of poverty, overcrowded households, poor sanitation, and weak health systems in developing countries compared to industrial countries.
I then applied four scenarios to this data: first a uniform infection rate of 10 per cent with a mortality rate of .05 of the parenting age group; second a uniform infection rate of 10 per cent with an increased mortality rate of 1 per cent; third an infection rate 30 per cent; and fourth an infection rate of 60 per cent, which is the figure often cited as the high point at which time herd-immunity kicks in, in a specific community, and the virus stops spreading within that community.
Table 3 presents four scenarios of how COVID-19 could play out in the three regions.
Chart 1:
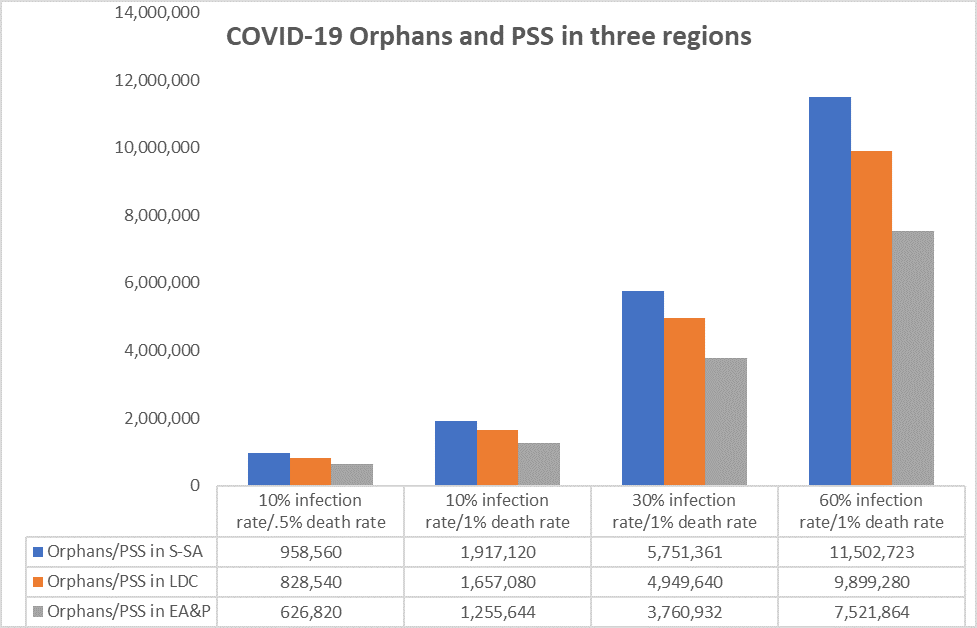
Column one shows that an infection rate of 10 per cent in each of the three regions, with a mortality rate of .5 per cent of adults 20-49 years of age, could result in up to 958,560 children being orphaned in Sub-Saharan Africa; up to 828,420 children being orphaned in Least Developed Countries; and up to 626,820 children being orphaned in developing countries, excluding China, in East Asia and the Pacific. Columns two, three and four show increased numbers of orphans based on a mortality rate of 1 per cent with infection rates of 10 per cent in column two, 30 percent in column three and 60 per cent in column four. The data in scenario four present a grim picture with the number of children becoming orphans increasing to 11, 502,723 in Sub-Saharan Africa.
These figures are not projections. They are scenarios based on the limited data available now. The indicator I have used is a crude one and more rigorous analysis it required.
However, counting the mortality rates of adults and children, particularly in resource poor countries where child protection services are limited or non-existent, provides a useful indicator for estimating both the number of children that could be orphaned and the number of children requiring psychosocial support as part of the broader humanitarian response to the pandemic.
Let’s bring this blog to a close with a final word from the United Nations Secretary-General, António Guterres, during his remarks on COVID-19: A Call for Solidarity: “We are facing a global health crisis unlike any in the 75-year history of the United Nations — one that is spreading human suffering, infecting the global economy and upending people’s lives.”
Bruce Grant, April 2020
Upcoming blogs will cover the challenges faced by child protection actors in maintaining resources for existing child protection interventions and challenges faced in mobilization additional resources in the era of COVID-19. I would also like to look at the impact of the pandemic on specific groups of children such as girls and young women and children in juvenile justice facilities.
Ideas for future blogs are most welcome as are offers to collaborate on writing blogs and think pieces relevant to child protection in developing countries.
Below is a round-up of some main resources available on child protection and COVID-19.
On 25 March the United Nations Secretary General launched the Global Humanitarian Response Plan COVID-19. The Plan recognises the risk of orphanhood noting that children are at risk of losing or being separated from primary caregivers due to quarantine or confinement measures are at increased risk of neglect, abandonment, violence and exploitation. In addition, the plan notes that children may suffer mental health and psychosocial impacts, and malnutrition. The Plan responds to gender-based intimate partner violence which is expected to increase due to the containment measures, compounded by the disruption of support services. Under Strategic priority two, UNICEF is charged with ensuring that children and women have continued access to essential health care, education, child protection and gender-based violence services. UNICEF is also a co-lead for social protection which is critically important for children and particularly households with orphans.
The Alliance for Child Protection in Humanitarian Action has released a Technical Note on the Protection of Children during the Coronavirus Pandemic outlining how the spread of COVID-19 can expose children to protection risks and providing a road map for reducing these risks through the application of the 2019 Minimum Standards for Child Protection in Humanitarian Action (CPMS). The Technical Note provides practical guidance for child protection practitioners to better respond to the child protection risks during the pandemic.
The Better Care Network is an international network of organizations committed to supporting children without adequate family care around the world. It is a collaboration of the many global child protection organisations with funding support from the US. It has created a resource section on the response to the COVID-19 pandemic as it relates to child protection and children's care. A review of the broader site and its key documents, particularly the number of children unnecessarily placed in institutions is a timely reminder that no matter how many children may lose one or both parents to the pandemic, institutional care is not an appropriate response.
The Global Partnership to End Violence Against Children continues to be a source for up to date resources for the child protection sector. A new set of resources and key messages on parenting have been produced by parenting experts from a number of organizations The experts include UNICEF, WHO, USAID, US Centers for Disease Control, Parenting for Lifelong Health, Internet of Good Things and the Global Partnership to End Violence Against Children. The resources will be available in more than 30 languages over the coming weeks. Social media materials promoting key messages are also available for you to use and share.
UNICEF, has gone into overdrive providing core social messaging particularly around hygiene and parenting. It is also strengthening supply chains for essential health supplies and for water and sanitation and strengthening delivery mechanisms for social protection assistance including social cash transfers. With now more than 80 percent of schools globally impacted by the pandemic UNICEF is aiming to help children continue their learning while keeping schools safe. UNICEF is the go-to site to understand the impact and drivers of risk for all children and young people in the context of COVID-19. UNICEF global situational report number 1 on novel coronavirus.
Updated 4 April 2020. The text for table 1 has been revised to clarify that a mortality rate of 0.5 and 1 per cent were used to show that even a small death rate in the parenting age group could have severe consequences for children.